While xylitol in a nasal spray is marketed as a nasal wash that is not what it does. Aggressively washing the body—any part of the body—can remove the helpful and friendly microbes that provide many of our defenses. We learned that over the last few decades beginning with Bill Costerton’s telling us about our helpful biofilms. More about him in a bit. Our environments need cleaning but soap and water on your hand to wash the rest of you is aggressive enough. In the nose we have a defensive cleaning mechanism in the combination of the mucus—that attaches to all the pollutants—and the microscopic hairs—the cilia, that sweep it out. Everyone has this defense, but it’s mostly handicapped. We developed it over thousands of years living outdoors where the environmental humidity is higher that what’s in our homes and offices, which is why it’s handicapped.
The best study showing this is by A.V. Arundel and colleagues (the whole article is at PMCID 1474709 at pub med)
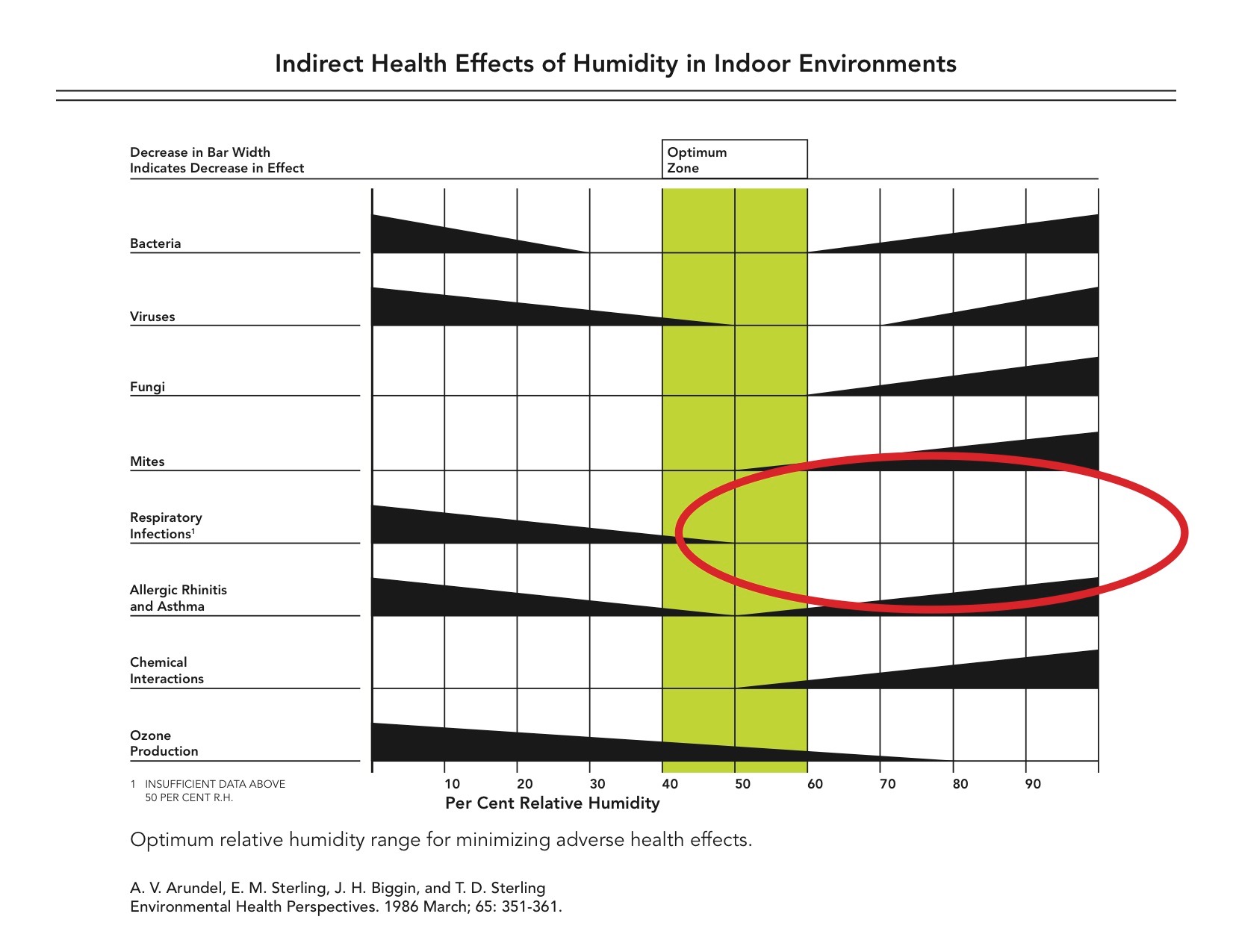
There are several points to remember here: all respiratory conditions are better when a person is in the optimal range of 40-60% relative humidity; that optimal range is what we adapted to, and a key point is that respiratory infections are not enough to measure when the humidity is greater than 50%.
So this level of humidity works. Why does it work? It works because both the cilia and the mucus need water in order to do what they do. The cilia need water in which to sweep. That’s provided by the airway surface fluid. This fluid also provides the water needed for the concentrated mucus secreted by goblet cells to absorb in order to become the viscous stuff that works. And this microscopic layer of water doesn’t need much—even 20 to 30% more humidity in the air we breathe is enough. But if it’s not provided the system stops working. Fisher & Paykel is a company in New Zealand that makes humidifiers for CPAP machines. Ample humidification is in their interest so they made a video showing how the cleaning stops without it. It’s on YouTube but changes often so search “mucocilliary” and “humidity,” and if that’s not enough add “Fisher & Paykel.”
When this system is working we are protected from most infections; Arundel could not document enough respiratory infections when humidity was over 50%. Why are we not old when sent home to quarantine with COVID to do so in a small room with a humidifier? Lot’s of other questions arise with similar unknowns. One major one is the fact that interfering with microbial adherence stops contagion; if the microbe is trapped in the mucus it’s just washed out—and on the way out it is recognized by immune white blood cells and lymphatic tissue that trigger immunity. That’s how it should happen—immunity without getting sick. And that’s how it happens in about a third of our population, but there is no one trying to figure out what this third shares to make them so blessed. Why not? Likely they work outside where the humidity is more often in Arundel’s optimal zone, but we don’t know for sure because no one is looking.
Joe Zabner wanted to market nebulized xylitol for his cyclic fibrosis patients and showed how xylitol worked osmotically to pull water into the nose. He did about half a dozen studies for the FDA before he realized his efforts making a food into a drug would not reward him with enough financial return to pay for the studies. If you have bronchitis or a deep cough and have a nebulizer add some xylitol for better results. It works in both the nose and the lungs by restoring the airway environment to the optimal zone. That’s one big reason why it works.
It helps in other ways as well. Bill Costerton was one of the main reasons we don’t tell women to douche any longer. He recognized the value of our protective and friendly bacteria, and that washing them out eliminated their protection. Those microbes and their protection are on our skin as well as—in abundance—at our vulnerable openings. Washing them out is seen as part of our war on microbes, but it increases infections. This has been shown with douching and even with users of a neti-pot. But there are ways that help without crippling our defenses. Long ago, in 1977, Costerton wrote and article for Scientific American, “How Bacteria Stick” (available online: search title and Costerton) in which he introduces another ignore element in today’s drug research.
That element is the long chains of sugars and sugar complexes that coat all of the proteins in our bodies. They’re called glycans, and all of the proteins you read about and hear on the news are properly called glycoproteins. Costerton describes it as a glycocalyx that essentially covers the microbe, and while he saw them only in bacteria they also cover viruses. Both the SARS-CoV-2 virus and its target receptor, the ACE2 inhibitor, are heavily glycosylated. In both bacteria and viruses the adhesion that begins infection is between the glycans on both us and the microbe. Costerton’s article, published in January of 1978, describes three ways to interfere with this process and suggests them as a source for how to cope with infections. But no one has pursued his valid suggestions. Why not?Most likely for the same reason Zabner gave up on the FDA; the glycans are sugars and sugar complexes that cannot be modified, patented, controlled and profitable, so they can be made into FDA approved drugs. Glycans, and other sugars, or molecules that can interfere with adhesion as Costerton suggests are more likely to be foods with drug effects. I call the Hippocratic drugs because he told us our food should be our drugs.
Xylitol is such a food and it fits into all three of Costerton’s scenarios. Xylose is a glycan and xylitol’s parent sugar. It is often the glycan that binds with the protein on the cell surface. Costerton’s first option is blocking the process of glycosylation and xylitol can get into the cell to block—by competitive inhibition—this process. His second option is interfering with the lectin—a protein that mediates glycan adhesion. Xylitol’s advantage is its flexibility; while all of the glycans are fixed in their structure and so provide a stable informative matrix, xylitol can shapeshifter to look like many of the glycans, even to the point of blocking a lectin. Costerton’s third is his favored; it’s blocking adherence at the binding site, which is the best explanation for what xylitol has been observed to do with both bacteria and viruses, including the Respiratory Syncytial Virus and SAR-CoV-2.
In discussing this last method Costerton concludes:
One attractive aspect of an antibiotic directed against the glycocalyx is that it need not enter the host cells or the bacterial cells. thereby avoiding two common problems in antibiotic therapy: toxicity to host cells and the induction of bacterial resistance based on changes in the permeability of the bacterial-cell membrane.
The importance of this observation cannot be ignored; it doesn’t hurt our friendly microbes, and it’s a means of negotiating an end to our war on microbes. Again we ask why it’s ignored, and the unstated answer from the system is, “it is not in our financial interest.”
But if you are a part of the public, instead of part of the system, it’s in your interest to be healthy.
So do what my mom told me to do every day she sent me off to school:
KEEP YOUR NOSE CLEAN!
You mentioned adding xylitol to a nebulizer for bronchitis or deep cough, but did not mention how much is safe.
Sorry for the tardy reply. The reply depends on how much you use. Spaying Xlear in the mouth while inhaling would likely work because of the limited amount. Xlear is twice the normal body’s concentration so I would not want to use more than one cc in a nebulizer. Zabner stuck with an isotonic solution in his nebulizer use. That’s close to making Xlear at half strength. The benefit of the concentration in small doses is that it brings the airway back to an optimal environment.
If this is all greek to you it’s explained better in my book, Common Sense Medicine; Healing the Body from the Inside Out, available at Amazon.
Cheers, Lon
I just use Xlear. 2 or 3 ccs in the nebulizer cup lasts about 3 or 4 minutes. Alternatively spray your mouth with a deep inhalation also delivers it to your lungs.